

COURSE 001
COURSE 001 FREE ACCESS
Introduction To Testosteronology®
FOUNDATION
Learn how testosterone and broader androgen care evolved into a complex clinical field, and why modern clinicians need a disciplined framework for diagnosis, prescribing, monitoring, interdisciplinary coordination, and harm reduction across real-world patient presentations.
PROGRAM Testosteronology® Professional Education Program, Testosteronology Society®
ESTIMATED TIME TO COMPLETE 45 Minutes Reading + 36 Minute Video
TARGET AUDIENCE Clinicians treating patients with testosterone deficiency, androgen-related conditions, and broader hormonal health challenges.
COURSE FORMAT Evidence-informed clinical education module including text, video, and diagrams
FACULTY DISCLOSURE Authors and reviewers include Thomas O’Connor, M.D., and Omar Hajmousa, PharmD. This educational material is designed as an independent clinical training course. Formal CME accreditation cannot currently be claimed.
CONTENT DISCLOSURE This educational material was developed with editorial assistance from AI technology and then reviewed, revised, and verified by the Testosteronology Society® faculty to ensure accuracy, clinical appropriateness, and educational value.
COURSE PREREQUISITES Courses are structured to be taken in sequence so clinicians can build a coherent clinical framework. Individual courses may be revisited anytime for refresher learning or when a patient presentation relates to a topic addressed in the curriculum.
IMPORTANT NOTE The course material is provided for general educational and informational purposes only. It is not intended to serve as medical advice, diagnosis, or treatment recommendations for any specific individual.
COURSE 001 OVERVIEW
Androgen medicine cannot be reduced to symptoms, serum levels, and dose titration without capturing how patients actually present in practice. Testosterone entered medicine through a major endocrine breakthrough in 1935. Over the following decades, its clinical use was shaped by pharmaceutical development, athletic misuse, anti-doping policy, federal regulation, and the later rise of commercial testosterone clinics.
Testosteronology® is presented here as a framework for managing androgen care. The goal is not to glorify older eras of hormone therapy or to condemn every modern access model, but to understand why the field became fragmented and why responsible care now has to include diagnostic discipline, structured monitoring, documentation quality, interdisciplinary judgment, and harm reduction when patients are already using anabolic agents or other Image and Performance enhancing Drugs (IPEDs).
COURSE 001 LEARNING OBJECTIVES
After completing this course, clinicians should be able to:
① Explain how the discovery of testosterone and the later development of anabolic-androgenic compounds shaped modern androgen medicine.
② Describe how therapeutic use, athletic misuse, anti-doping structures, and federal regulation changed the clinical and cultural status of testosterone and related agents.
③ Recognize why decades of medical reluctance contributed to fragmented androgen care and helped create the modern TRT and wellness-clinic marketplace.
④ Define Testosteronology® as a medicine-first clinical discipline that integrates internal medicine, endocrinology, cardiometabolic risk management, hematology, psychiatry, reproductive considerations, and longitudinal monitoring.
⑤ Explain why modern androgen care requires more than prescribing, including diagnostic discipline, structured follow-up, documentation quality, interdisciplinary coordination, and harm-reduction thinking for patients with ongoing anabolic steroid or IPED exposure.
COURSE 001 TOPICS
The following topics will be covered in the course text, video, diagrams or downloadable documents:
① Why This Course Comes First
② The Discovery Of Testosterone In 1935
③ The Golden Era Of Anabolic Steroid Development
④ When Androgen Medicine Split Between Therapeutics And Performance
⑤ The 1990 Regulatory Turning Point
⑥ Why Traditional Medicine Pulled Back
⑦ The Rise Of TRT Clinics, Wellness Models, And Telemedicine
⑧ The Current Clinical Crisis In Androgen Care
⑨ Defining Testosteronology®
⑩ The Mission Of This Training Program
“Testosteronology® is the modern clinical discipline dedicated to understanding, prescribing, and safely managing testosterone and androgens across the full spectrum of human health and performance.”

Thomas O'Connor, M.D.
Become an Associate Testosteronologist® and unlock the complete 14-Course Educational Program from the Testosteronology Society® to advance your clinical knowledge in testosterone and androgen medicine.

Testosteronology® Professional Education Program + One Year Society Membership
◉ Access To The 14 Course Testosteronology® Professional Education Program
◉ Access To The Official Society TRT Guidelines
◉ Access To The Topic Presentations Library
◉ Access To Grand Rounds Recording Library
◉ Monthly Live Q&A Training Group Session
◉ Ongoing Clinical Education Updates
◉ Weekly Testosteronology Society® Insights Newsletter
◉ Professional Testosteronology Society® Member Designation
◉ Access To The Testosteronology Society® Website
001 Introduction To Testosteronology®
36 MINUTE COURSE TRAINING VIDEO
With Thomas O'Connor, M.D. Founder / CEO Testosteronology Society®
Video Lesson Takeaways
◉ Androgen medicine requires more than symptom review, serum interpretation, and dose adjustment, because responsible care depends on understanding how patients actually present across complex real-world clinical settings.
◉ The synthesis of testosterone in 1935 established the scientific and clinical foundation for modern androgen medicine by converting earlier observations about testicular function into a defined and measurable hormone signal.
◉ Many anabolic-androgenic compounds originated in legitimate therapeutic development, but their later expansion into athletics, bodybuilding, and recreational performance enhancement changed both public perception and medical culture around androgen use.
◉ Anti-doping systems and controlled-substance regulation influenced far more than sport and legal oversight, because they also increased clinician caution, stigma, and reluctance to manage patients with complex androgen exposure histories.
◉ The withdrawal of many traditional medical settings from difficult androgen cases helped create the modern expansion of TRT clinics, wellness models, and telemedicine-based hormone care.
◉ Safe and effective androgen care requires a broader medicine-first framework that incorporates exposure history, cardiometabolic and hematologic monitoring, psychiatric and reproductive context, structured follow-up, and harm-reduction thinking.
COURSE 001 TEXT
① Why This Course Comes First
Testosteronology® is a field of internal medicine that sits at the intersection of endocrinology, cardiometabolic medicine, psychiatry, reproductive health, and long-term risk management. Without understanding how androgen medicine developed historically and why current practice patterns became fragmented, clinicians risk applying simplified treatment frameworks to patients whose presentations are far more complex. Establishing the historical and clinical context allows later courses to focus on diagnosis, pharmacology, monitoring strategies, and harm-reduction frameworks with a clearer understanding of how modern androgen care evolved.
② The Discovery Of Testosterone In 1935
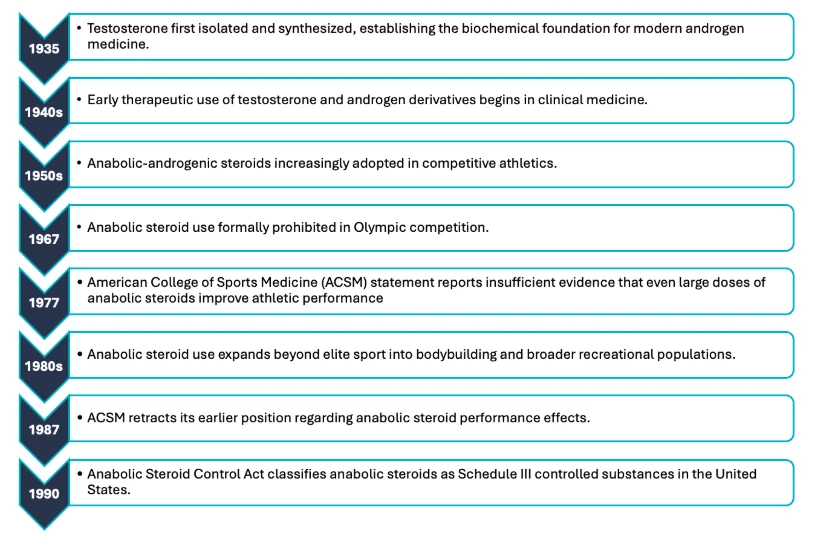
Modern testosterone pharmacology emerged in 1935, when testosterone was first synthesized. This converted prior observations about testicular function into a defined chemical signal that could be measured and used clinically. Independent work by Laqueur, Butenandt, and Ruzicka established testosterone as the principal male androgen and enabled therapeutic development.[1,2]
Testosterone entered medicine as a defined physiologic signal with broad systemic relevance. Its effects extend beyond reproductive biology into muscle, erythropoiesis, body composition, metabolism, and behavior. Modern discussion often oversimplifies testosterone, but the field originated as rigorous hormone science and still requires that level of clinical discipline.
③ The Golden Era Of Anabolic Steroid Development
After 1935, pharmaceutical research expanded rapidly as investigators explored androgenic and anabolic effects across multiple disease states such as muscle wasting, anemia, delayed puberty, osteoporosis, chronic illness, and other catabolic states in which anabolic signaling was thought to improve clinical outcomes. This period included development of injectable esters, oral derivatives, and other delivery strategies aimed at improving durability, practicality, and tissue-specific effects. [1-3]
During this period of rapid pharmaceutical development, androgen pharmacology also became organized around three broad structural families that remain clinically relevant today: testosterone-derived steroids, 19-nor derivatives, and dihydrotestosterone (DHT)-derived compounds. These categories reflect attempts to modify anabolic and androgenic effects through chemical structure while preserving therapeutic usefulness. Their later misuse altered public perception, but their therapeutic origins remain clinically relevant [1,3].
④ When Androgen Medicine Split Between Therapeutics And Performance
Androgen use diverged into two domains: therapeutic use and performance enhancement. As anabolic agents expanded in medicine, they also expanded into competitive sport and later into bodybuilding and recreational fitness. That parallel growth changed the public meaning of these drugs. [3,4,8]
That shift was later formalized through anti-doping institutions. The IOC Medical Commission was established in 1967, and WADA was established in 1999 to coordinate anti-doping efforts internationally. Those bodies were created for sport, but their influence reached far beyond elite competition. They helped shape the broader cultural and professional story around anabolic agents, and that story still affects how patients, clinicians, and regulators think about androgens today. [3-5]
Clinically, the practical consequence is easy to underestimate. Many clinicians inherit this field already loaded with controversy before they ever encounter pharmacology. That means testosterone and anabolic agents are often discussed through the language of scandal or fear long before they are discussed as medicines, exposures, or physiologic stressors.
⑤ The 1990 Regulatory Turning Point
The Anabolic Steroid Control Act of 1990 placed anabolic steroids into Schedule III of the Controlled Substances Act, increasing penalties for steroid trafficking and imposing stricter production and recordkeeping requirements.The legislation followed growing public concern regarding anabolic steroid use in competitive athletics, including high-profile doping scandals during the 1980s Olympic era. [3]
Controlled-substance status does more than change pharmacy rules. It changes clinician behavior by raising the stakes of prescribing, documentation, storage, and professional scrutiny. In some settings this pressure sharpens discipline. In androgen medicine, it also contributed to avoidance, as many clinicians became less willing to engage patients with prior steroid exposure, mixed goals, or perceived legal and reputational risk. The field remained legitimate, but the comfort level around it narrowed. [3,8,11]
⑥ Why Traditional Medicine Pulled Back
From the passage of the Anabolic Steroid Control Act in 1990 through the COVID-19 pandemic era, many clinicians became increasingly cautious about diagnosing or managing androgen-related conditions.Testosterone therapy remained part of endocrinology, internal medicine, urology, and primary care, but many clinicians were reluctant to take ownership of more complex androgen cases. Data from large survey cohorts of men using anabolic androgenic steroids show that this gap is not theoretical. A majority of respondents did not disclose use to their clinicians, commonly citing concern for judgment, limited clinician familiarity, and potential repercussions. Among those who did disclose, more than half reported feeling stigmatized. These dynamics interfere with accurate history-taking, weaken trust, and disrupt continuity of care. [11]
At the same time, formal testosterone guidelines continued to emphasize diagnostic rigor, informed discussion of risk and benefit, and structured follow-up. That was an important advance, but guidelines alone could not resolve the broader gap. Patients were presenting with prior cycles, supraphysiologic dosing histories, self-directed post-cycle therapies, fertility concerns, sleep disorders, obesity, polypharmacy, and psychiatric complexity. When traditional systems did not integrate these realities effectively, patients often sought guidance outside conventional medical settings [6,7].
⑦ The Rise Of TRT Clinics, Wellness Models, And Telemedicine
This expansion did not occur in isolation. As many traditional clinicians became increasingly reluctant to manage complex androgen cases, a clinical vacuum developed in which patient demand for testosterone therapy and androgen management remained present while medical ownership of the field became less consistent. TRT clinics, anti-aging practices, and commercial hormone programs expanded into that gap, often emphasizing accessibility and convenience but sometimes adopting standardized treatment pathways that did not fully account for patient complexity. [6,7, 8,11]
Telemedicine accelerated that shift, particularly during the COVID-19 pandemic when regulatory flexibility and access constraints rapidly expanded remote care. This period made both the strengths and limitations of the field more visible. Regulatory agencies have also recognized the need to balance access with oversight. HHS and DEA announced in January 2026 that key telemedicine flexibilities for controlled substance prescribing were extended through December 31, 2026 while permanent rules are finalized. [9,10]
⑧ The Current Clinical Crisis In Androgen Care
Today, millions of individuals worldwide use testosterone therapy, anabolic steroids, or other image- and performance-enhancing drugs (IPEDs). In some clinical settings this complexity has been compounded by standardized prescribing patterns that extend beyond testosterone therapy alone. Patients may receive layered treatment protocols that include aromatase inhibitors, selective estrogen receptor modulators, gonadotropins, peptides, and other adjunctive agents. These patterns illustrate how androgen care can evolve into multi-drug exposure systems that require careful clinical interpretation and structured monitoring rather than isolated hormone replacement decisions. [8,9]
The clinician is therefore not evaluating a single hormone in isolation. The clinician is evaluating an exposure system. If care is approached only through a standard TRT framework, patients with prior or ongoing IPED exposure can appear inconsistent and difficult to manage. If care is approached only through a misuse framework, appropriate testosterone therapy can become stigmatized and underdelivered. [6-9,11]
⑨ Defining Testosteronology®
Testosteronology® is presented as a clinical approach to managing androgen care in patients with complex exposure histories. It is not limited to standard testosterone replacement and it is not defined by prescribing alone. The focus is on structured evaluation and management, including exposure history, laboratory interpretation, cardiometabolic risk, psychiatric context, reproductive considerations, sleep, documentation, and appropriate referral when needed.
The discipline also reflects a collaborative model in which multiple healthcare specialties contribute to the safe management of androgen exposure and therapy. This reflects the reality that androgen related decisions can affect erythrocytosis, blood pressure, sleep disordered breathing, fertility, mood, lipid profiles, and long term cardiovascular risk simultaneously [6-8].
A practical framework for managing androgen therapy must therefore incorporate structured cardiometabolic and hematologic monitoring. One example referenced in the training program is the ABCDS™ framework, which emphasizes attention to glycemic context and hemoglobin A1c, blood pressure and renal health, cholesterol and cardiovascular disease, and differentiation of androgen-related erythrocytosis from primary hematologic disorders. These domains illustrate how androgen therapy intersects with broader internal medicine considerations rather than existing as a narrow endocrine intervention.
Before addressing specific therapies and management strategies, it is necessary to understand how androgen medicine developed and why current clinical gaps persist. The field has been shaped by scientific progress, nonmedical use, regulatory pressure, and expansion of access through commercial and telemedicine models. These forces have produced a patient population that often does not fit within traditional testosterone deficiency frameworks.
As a result, androgen care requires a broader clinical approach. Evaluation must extend beyond serum levels and symptom checklists to include exposure history, risk assessment, and structured follow-up. Many patients present with prior or ongoing use of anabolic steroids or other IPEDs, along with overlapping cardiometabolic, psychiatric, and reproductive considerations. This context is necessary before applying specific therapies or management decisions.
⑩ The Mission Of This Training Program
The mission of this training program is to provide clinicians with a structured framework for approaching androgen care in a field that has become clinically fragmented. The goal is not only to teach prescribing mechanics, but to improve diagnostic reasoning, longitudinal monitoring, interdisciplinary coordination, and harm-reduction strategies for patients who may already be using anabolic steroids or other IPEDs.
An additional objective is to promote a nonjudgmental clinical approach to patients with androgen exposure histories. Many individuals present after prior unsupervised or performance-oriented use, and effective care requires ethical engagement rather than stigma.
COURSE 001 SUMMARY
Introduction To Testosteronology® establishes the foundation for understanding androgen medicine by tracing the history of testosterone from its discovery in 1935 through its evolution across therapeutic use, athletic misuse, regulation, and the rise of modern TRT and wellness models. It explains how these forces fragmented the field and created a patient population that often presents with overlapping exposures, comorbidities, and symptom narratives that simplified prescribing models were never designed to handle. The course introduces Testosteronology® as a structured, medicine-first clinical discipline, one that applies the diagnostic rigor of internal medicine to androgen care, integrates the ABCDS™ monitoring framework as a practical tool across every patient encounter, and treats harm reduction as a medical standard rather than a philosophical option. Clinicians who complete this program should leave not just with new information, but with a different way of thinking about what androgen medicine actually requires and why the patients who need it most are precisely the ones most often failed by shortcuts.
COURSE 001 EVALUATION
Introduction to Testosteronology®
This self-evaluation helps you confirm your understanding of the course material. There is no passing or failing score — it is a tool for reflection and review.
Course 001 Reviewed
You have completed the self-evaluation for Introduction to Testosteronology®. Review any flagged topics in the course content above before proceeding.
Question Summary
COURSE 001 REFERENCES
- Nieschlag E, Nieschlag S. The history of discovery, synthesis and development of testosterone for clinical use. Eur J Endocrinol. 2019;180(6):R201-R212.
- Freeman ER, Bloom DA, McGuire EJ. A brief history of testosterone. J Urol. 2001;165(2):371-373.
- Kanayama G, Pope HG Jr. History and epidemiology of anabolic androgens in athletes and nonathletes. Mol Cell Endocrinol. 2018;464:4-13. doi:10.1016/j.mce.2017.02.039
- International Olympic Committee. IOC Medical Commission: History and Development. Lausanne, Switzerland: International Olympic Committee; 1967.
- World Anti-Doping Agency. A Brief History of Anti-Doping. Montreal, Canada: World Anti-Doping Agency; Updated 2023.
- Bhasin S, Brito JP, Cunningham GR, et al. Testosterone therapy in men with hypogonadism: an Endocrine Society clinical practice guideline. J Clin Endocrinol Metab. 2018;103(5):1715-1744.
- Mulhall JP, Trost LW, Brannigan RE, et al. Evaluation and management of testosterone deficiency: AUA guideline. J Urol. 2018;200(2):423-432.
- Bonnecaze AK, O’Connor T, Burns CA. Harm reduction in male patients actively using anabolic androgenic steroids and performance-enhancing drugs: a review. J Gen Intern Med. 2021;36(7):2056-2064.
- Dubin JM, Fantus RJ, Halpern JA. Testosterone replacement therapy in the era of telemedicine. Int J Impot Res. 2022;34(7):663-668. doi:10.1038/s41443-021-00498-5
- US Department of Health and Human Services. HHS and DEA extend telemedicine flexibilities for prescribing controlled substances through 2026. Published January 2, 2026.
- Bonnecaze AK, O’Connor T, Aloi JA. Characteristics and attitudes of men using anabolic androgenic steroids: a survey of 2385 men. Am J Mens Health. 2020;14(6):1557988320966536. doi:10.1177/1557988320966536
Recommended Grand Rounds Case Reviews


Testosteronology® Professional Education Program