
Testosterone Therapy: Core Clinical Framework
COURSE 4-2
Testosterone Drug Formulations: Injections, Transdermal Agents, Pellets, and Oral Formulations
Learn testosterone drug formulation including injections, transdermals, pellets, and oral agents to select the best administration method for patient success.
PROGRAM Advanced Clinical Training Program, Testosteronology Society™
ESTIMATED TIME TO COMPLETE 45 Minutes Reading + 30 Minute Video
TARGET AUDIENCE Clinicians treating patients with testosterone deficiency, androgen-related conditions, and broader hormonal health challenges.
COURSE FORMAT Evidence-informed clinical education module including text, video, and diagrams
FACULTY DISCLOSURE Authors and reviewers include Thomas O’Connor, MD, PA, and Omar Hajmousa, PharmD. This educational material is designed as an independent clinical training course. Formal CME accreditation can not currently be claimed.
CONTENT DISCLOSURE This educational material was developed with editorial assistance from AI technology and then reviewed, revised, and verified by the Testosteronology Society™ faculty to ensure accuracy, clinical appropriateness, and educational value.
COURSE PREREQUISITES Courses are structured to be taken in sequence so clinicians can build a coherent clinical framework. Individual courses may be revisited anytime for refresher learning or when a patient presentation relates to a topic addressed in the curriculum.
IMPORTANT NOTE The course material is provided for general educational and informational purposes only. It is not intended to serve as medical advice, diagnosis, or treatment recommendations for any specific individual.
Course Overview
Formulation choice is one of the most important clinical decisions in testosterone therapy because treatment success depends on more than achieving a laboratory target. The same nominal weekly exposure can produce very different patient experiences depending on pharmacokinetics, execution of the regimen, and the ability to monitor follow-up consistently. Cost also matters because affordability often determines whether a plan remains durable in real practice. Current guidelines and review literature support the idea that route, timing, adherence, and monitoring all materially influence symptom stability and safe long-term care. [1-4]
This course reviews testosterone formulations through a practical clinical lens focused on pharmacokinetic reasoning, adherence realities, lab timing, and side-effect interpretation. A central theme is that many apparent testosterone problems are actually delivery-system problems, especially when volatility, poor technique, missed doses, or inconsistent monitoring are mistaken for treatment failure. Clinicians who understand how formulation choice shapes follow-up are better positioned to troubleshoot instability without reflexively escalating dose. [1-5]
Learning Objectives
After completing this course, clinicians should be able to:
➀ Explain how pharmacokinetics, peaks, troughs, and steady state influence testosterone therapy outcomes.
➁ Compare common testosterone drug formulation using practicality, tolerability, and monitoring needs.
➂ Recognize when symptoms reflect drug formulation instability rather than inadequate total exposure.
➃ Match a testosterone formulation to patient lifestyle, adherence patterns, and clinical risk.
➄ Apply a structured approach to monitoring, troubleshooting, and switching testosterone formulations when treatment becomes unstable or poorly tolerated.
Course Topics
The following topics will be covered in the course text, video, diagrams or downloadable documents:
➀ Why Drug Formulation Choice Drives Outcomes
➁ Core Pharmacokinetics, Lab Timing, And Steady State
➂ Injectable Testosterone And Pellets
➃ Transdermal Therapies
➄ Oral Testosterone Formulations
➅ Matching Formulation To Patient Lifestyle And Adherence
➆ Monitoring, Side Effects, And Switching Strategies
“The delivery system is not a minor detail after the diagnosis is made. It is one of the main determinants of whether treatment will feel smooth, chaotic, convenient, unsustainable, or unsafe. Good androgen care means choosing the route the patient can actually live with and then monitoring it in a way that produces interpretable medicine.”

Thomas O'Connor, M.D.
The full training course, including the content outlined and training video, is viewable only with an active Testosteronology Society™ Membership.
4-1 Testosterone Drug Formulations: Injections, Transdermal Agents, Pellets, and Oral Formulations
27 MINUTE COURSE TRAINING VIDEO
With Dr. Thomas O'Connor Founder / CEO Testosteronology Society™
Video Lesson Takeaways
◉ Testosterone care is moving out of the era where it can be treated as a minor part of general endocrinology, internal medicine, or urology.
◉ Women are now clearly part of testosterone care, which makes diagnostic standards, evidence review, and treatment caution even more important.
◉ Testosteronology® is framed here as a subspecialty of internal medicine rather than a surgical field.
◉ Prostate disease, BPH, and prostate cancer still require direct collaboration with urologists and cancer specialists.
◉ Managing testosterone and androgens is described as too complex for a cookie-cutter clinic model or casual protocol-based treatment.
◉ The androgen world includes more than prescribed TRT because clinicians also have to understand the broader spectrum of androgen and steroid exposure that patients bring with them.
◉ Androgen medicine crosses multiple systems at once, including skin, psychiatric health, cardiovascular risk, hematology, and sleep-related breathing problems.
◉ Androgen-induced erythrocytosis remains a real example of how much is still unsettled, including what the right management threshold should be and whether routine phlebotomy answers the problem.
COURSE TEXT
➀ Why Drug Formulation Choice Drives Outcomes
In clinical practice, formulation choice often determines whether testosterone therapy feels stable or erratic. Patients rarely present by saying their average exposure is inadequate. They present with fatigue late in the dosing interval, irritability after administration, sleep disruption, edema, acne flares, or a sense that treatment works briefly and then fades. Those complaints are often clues to the shape of the exposure curve rather than proof that total weekly exposure is too low. Clinical guidance and formulation reviews consistently emphasize that route and schedule affect symptom pattern, adherence, and the interpretability of follow-up. [1-4]
A useful mindset is to treat delivery-system selection as a clinical matching problem. A formulation that fits a patient’s schedule, tolerance, privacy needs, and follow-up capacity is more likely to produce stable care than one that looks ideal on paper but repeatedly fails in real life. Patients with chaotic routines may struggle with daily transdermal therapy. Patients sensitive to peak-trough shifts may do poorly with longer injection intervals. Patients who cannot reliably execute the prescribed regimen can become quietly inconsistent, which can then trigger unnecessary dose escalation. [1-5]
➁ Core Pharmacokinetics, Lab Timing, And Steady State
Pharmacokinetics and lab timing matter because testosterone exposure changes over time after administration, and those changes influence both symptoms and interpretation. High peaks can produce adverse effects and make levels appear supratherapeutic on paper, while low troughs can create the impression that therapy wears off before the next dose. Mapping symptoms to the dosing interval gives clinicians more useful information than reading a hormone value in isolation. Symptom timing and laboratory timing together create the clinical picture. As a general rule, clinicians should standardize the draw point within the dosing interval and interpret future results against that same reference point. [1-5]
Reaching steady state is crucial for decision-making because early adjustments can cause clinicians to read transition noise as treatment failure. Dose and formulation changes should usually be interpreted only after an appropriate stabilization window, with the timing of follow-up labs and symptom review clearly documented. As a pharmacokinetic principle, steady state is generally approached after about five half-lives. For example, a formulation with an approximately 8-day half-life may not provide a stable interpretive picture until roughly 5 to 6 weeks have passed. This matters not only for immediate management, but also for keeping the chart intelligible for future clinicians. [1-5]
Below is a graph of drug X concentration versus time with an assumption of a 7-day half-life. The drug is dosed once weekly. Notice that steady state is where the drug concentration waves consistently between a certain peak and trough.
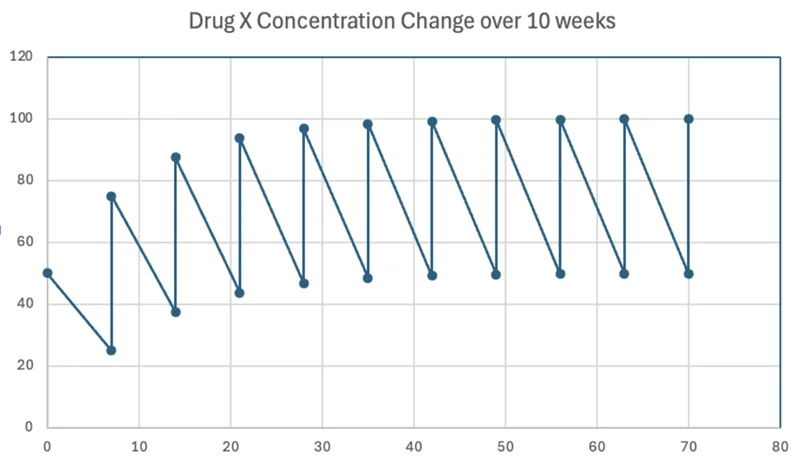
Figure 1. Conceptual representation of drug accumulation and steady-state pharmacokinetics assuming a 7-day half-life.
➂ Injectable Testosterone And Pellets
Injectable testosterone cypionate and enanthate remain among the most widely used treatment options because of their familiar pharmacokinetic profile, availability, and relative affordability. Their longer half-life can be an advantage, but it can also become a liability when interval selection produces excessive peaks and troughs. Another common mistake is assuming the patient already knows how to measure, administer, and store the medication correctly. Injection regimens are only as reliable as their execution, so technique education is not a minor detail. It is part of the treatment plan itself. [5]
Subcutaneous administration can be more comfortable and easier for some patients, and available evidence suggests pharmacokinetic performance that is broadly comparable to intramuscular administration in appropriate settings. While evidence does not show clear superiority of the subcutaneous route in efficacy, it can be a practical option when needle tolerance, convenience, or patient preference make intramuscular administration less appealing. [6]
Injectable testosterone undecanoate offers a long-acting option designed for extended dosing intervals under supervised office administration because of the boxed warning for pulmonary oil microembolism and anaphylaxis. Its pharmacokinetic profile can support therapeutic testosterone concentrations with dosing approximately every 10 weeks after the loading phase. The tradeoff is reduced flexibility. When adverse effects or misalignment appear, rapid adjustment is less practical than it is with shorter-acting injectable options. Office administration requirements and cost can also limit routine use. [7,9]
Pellets appeal to patients who want fewer administration events and less weekly or daily treatment friction. Their main advantage is adherence support through infrequent dosing. Their main limitation is low adjustability once implanted. Other risks include procedural issues such as extrusion, infection, bruising, and local discomfort, which is why pellets fit best in patients who value convenience and accept slower response to any needed adjustment. [5]
➃ Transdermal Therapies
Transdermal gels and creams can work very well when absorption and daily routine are consistent. Their major strength is smoother day-to-day exposure compared with wider-interval regimens, and they can be especially useful in patients who strongly prefer to avoid needles. Their major weaknesses are variability and cost. Skin conditions, sweating, bathing, application habits, and simple inconsistency can all change delivery enough to create unstable symptom narratives. Transfer to female household members and children is another important risk. In many cases, transdermal failure is behavioral or situational before it is pharmacologic. Before assuming the dose is inadequate, clinicians should first assess technique, routine consistency, and adherence. That counseling is often the difference between a formulation that appears ineffective and one that works predictably. [1-5]
Patches reduce transference concerns compared with gels, but they bring their own burdens. Adhesion problems, visibility, and local skin irritation are common reasons patients stop using them consistently. If the patch does not stay on reliably, or if the skin becomes irritated enough to reduce adherence, the patient is effectively receiving an erratic regimen even when the prescription itself is appropriate. [5]
➄ Oral Testosterone Formulations
Oral testosterone has re-emerged as a therapy option with the development of newer testosterone undecanoate products that rely on lymphatic absorption rather than the older 17-alkylated pathway associated with hepatotoxicity concerns. These newer agents now have FDA-approved roles in selected patients, but they also introduce practical limitations. Food timing, dosing frequency, blood pressure considerations, and cost can all reduce convenience or durability in real-world use. [8-11]
Reference guide to available testosterone delivery systems, dosing, and clinical pearls.
| Generic | Brand | Strength | Route | Half Life | Dosing | Pearls |
|---|---|---|---|---|---|---|
| Injectable | ||||||
| Testosterone Cypionate1*Compounding available with various carrier oils and excipients | Depo-Testosterone Azmiro |
200 mg/mL Or 100 mg/mL (less common) |
IM/SubQ | ~8 days | Starting dose for most men 70–100 mg every 5–7 days. Dose on an individual basis but frequency should be every 7 days at the longest. |
|
| Testosterone Enanthate2*Compounding available with various carrier oils and excipients | Delatestryl Xyosted |
200 mg/mL | IM/SubQ | 4.5–7 days IM* References unclear |
Dose on an individual basis but frequency should be every 7 days at the longest. Xyosted: Start 75 mg SubQ every 7 days. Target nadir 350–650 ng/dL total T. Increase by 25 mg/week if <350 and decrease by 25 mg/week if trough ≥650 ng/dL. |
|
| Testosterone Propionate14*Compounding available with various carrier oils and excipients | Commercially not available in the USA | 100 mg/mL | IM | 2–3 days per dosing regimen | 25–50 mg 2–3 times every week or 50–100 mg every other day in male athletes. | All information from Llewellyn's Anabolics 11th Edition — not a typical medical text. |
| Testosterone Undecanoate3 | Aveed Nebido (abroad) |
250 mg/mL | IM | ~3 months | 750 mg ×1 then 750 mg after 4 weeks (loading), then 750 mg every 10 weeks.5 In Europe/Abroad: 1 gm IM Q3 months. |
|
| Testosterone Esters5 | Sustanon 250 *Not available in the USA |
250 mg/mL | IM | Variable due to variety of esters | Pkg insert: Every 3 weeks Should be injected every 7 days14 |
|
| Pellets | ||||||
| Testosterone4 | Testopel | 75 mg/pellet | SubQ | Variable | 150–450 mg every 3–6 months6 |
|
| Topical / Transdermal | ||||||
| Testosterone Gel6*Compounding Available | Androgel / Vogelxo / Testim | 1% Androgel: 25 mg/2.5 g or 50 mg/5 g Vogelxo: 50 mg/5 g or 12.5 mg/pump Testim: 50 mg/5 g |
Topical | Steady state by day 2–3 | 50 mg QAM to shoulders and upper arms or abdomen; increase to 75 mg or 100 mg based on response. |
|
| Testosterone Pump6*Compounding Available | Androgel 1.62% | 20.25 mg/pump 20.25 mg/1.25 g or 40.5 mg/2.5 g |
Topical | — | 40.5 mg QAM to shoulders and upper arms or abdomen. Dose adjustments in 20.25 mg increments w/ the pump. |
|
| Testosterone Gel7*Compounding Available | Fortesta | 2% 10 mg/0.5 g |
Topical | — | 40 mg QAM to the thighs. Dose adjustments in 10 mg increments w/ the pump. |
|
| Testosterone Topical Solution8*Compounding Available | Axiron | 30 mg/1.5 mL | Topical | Steady state within 14 days | 60 mg QAM to the axilla using the applicator. Dose adjustments in 30 mg increments w/ the pump. |
|
| Testosterone Transdermal Solution9*Compounding Available | Androderm | 2 mg/day or 4 mg/day | Transdermal | 70 minutes | 4 mg Androderm system applied to the back, upper arms, abdomen or thighs QPM. Dose adjustments in 2 mg/day increments using the 2 mg patches. |
|
| Intranasal | ||||||
| Testosterone Nasal Gel10 | Natesto | 5.5 mg/0.122 g | Intranasal | — | 2 actuations (11 mg) TID |
|
| Oral | ||||||
| Testosterone Undecanoate Oral Capsule11,12,13 | Jatenzo / Kyzatrex / Tlando | Jatenzo: 158, 198, 237 mg Kyzatrex: 100, 150, 200 mg Tlando: 112.5 mg |
PO | 2 hours | Jatenzo: 158–396 mg BID with food Kyzatrex: 100–400 mg BID with food Tlando: 225 mg BID with food |
|
Or 100 mg/mL (less common)
Starting dose for most men 70–100 mg every 5–7 days. Frequency should be every 7 days at the longest.
- Gold Standard for TRT. Cheap and easy to access.
- Potential for high peaks and low troughs due to long half-life.
- Microdosing over a shorter interval can help with adverse effects but increases injection burden.
- Compounded variations can help with excipient and dose optimization.
References unclear
Frequency should be every 7 days at the longest. Xyosted: Start 75 mg SubQ every 7 days. Target nadir 350–650 ng/dL total T. Adjust ±25 mg/week based on trough.
- Insurance issues may arise with Xyosted if prescribed more frequently than every 7 days.
- Xyosted auto-injector is convenient but can be challenging to fine-tune dose.
25–50 mg 2–3 times/week or 50–100 mg every other day in male athletes.
All information from Llewellyn's Anabolics 11th Edition — not a typical medical text.
750 mg ×1, then 750 mg at 4 weeks (loading), then 750 mg every 10 weeks.5 In Europe: 1 gm IM Q3 months.
- Administered in office by a healthcare professional.
- Patients should be observed for 30 mins after administration.
Pkg insert: Every 3 weeks. Should be injected every 7 days.14
- Formulated in peanut oil — check for ALLERGIES.
- Contains 30 mg/mL propionate, 60 mg/mL phenyl propionate, 60 mg/mL isocaproate, 100 mg/mL decanoate.
150–450 mg every 3–6 months.6
- Pellets may extrude from the skin.
- Very difficult to adjust dose.
- 2 pellets for each 25 mg testosterone propionate required weekly.4
50 mg QAM to shoulders, upper arms, or abdomen. Increase to 75–100 mg based on response.
- Good option for fear of needles.
- Allow area to dry before dressing. Flammable.
- Avoid swimming/showering for at least 5 hours.
- Avoid contact with women or children.
40.5 mg QAM to shoulders, upper arms, or abdomen. Adjustments in 20.25 mg increments w/ the pump.
- Allow area to dry before dressing. Flammable.
- Avoid swimming/showering for at least 5 hours.
- Avoid contact with women or children.
40 mg QAM to the thighs. Adjustments in 10 mg increments w/ the pump.
- Allow area to dry before dressing. Flammable.
- Avoid swimming/showering for at least 2 hours.
- Avoid contact with women or children.
60 mg QAM to the axilla using the applicator. Adjustments in 30 mg increments w/ the pump.
- Flammable. Avoid swimming/showering for at least 2 hours.
- Apply deodorant BEFORE applying Axiron.
4 mg system applied to back, upper arms, abdomen, or thighs QPM. Adjustments in 2 mg/day increments using the 2 mg patches.
- Avoid swimming/showering for at least 2 hours.
- Itching is the most common adverse event.
- Fold patch in half to discard in household trash.
2 actuations (11 mg) TID
- TID dosing with Cmax of 1,044 ng/dL (40 mins post-dose) and Cmin of 215 ng/dL.
- Weak evidence of preserving fertility.15,16
- Discontinue temporarily with severe rhinitis.
Jatenzo: 158–396 mg BID with food
Kyzatrex: 100–400 mg BID with food
Tlando: 225 mg BID with food
- Different formulations are not interchangeable.
- No hepatotoxicity noted.
- PO is the easiest route of administration for adherence.
- See package inserts for recommended dosing and titrations.
- Testosterone cypionate injection [package insert]. Northstar Rx/AccessData. December 2022.
- XYOSTED (testosterone enanthate) [package insert]. AccessData (FDA). 2019.
- AVEED (testosterone undecanoate) [prescribing information]. AveedUSA.com. Latest.
- Testopel (testosterone pellets) [package insert]. Endo USA, Inc. Latest.
- Sustanon 250 (testosterone mixture) [patient information, UK]. Medicines.org.uk / EMC. Latest.
- AndroGel (testosterone gel) [package insert]. AccessData (FDA). 2013.
- Fortesta (testosterone topical gel) [dosage guide]. Drugs.com. ~July 2025.
- Axiron (testosterone topical solution) [product monograph]. AccessData (FDA) & DailyMed. Latest.
- Androderm (testosterone transdermal system) [prescribing information]. AccessData (FDA). May 2020.
- Natesto (testosterone nasal gel) [full prescribing information]. Natesto.com. ~2019.
- Jatenzo (oral testosterone undecanoate) [prescribing information]. Jatenzo.com. ~2023.
- Kyzatrex (oral testosterone undecanoate) [prescribing information]. AccessData (FDA). ~2022.
- Tlando (oral testosterone undecanoate) [prescribing information]. Tlando.com. Feb 2024.
- Llewellyn W. Anabolics. 11th ed. Jupiter, FL: Molecular Nutrition; 2017.
- Naelitz BD, Momtazi-Mar L, Vallabhaneni S, et al. Testosterone replacement therapy and spermatogenesis in reproductive age men. Nat Rev Urol. 2025;22(10):703–719.
- Ramasamy R, Masterson TA, Best JC, et al. Effect of Natesto on Reproductive Hormones, Semen Parameters and Hypogonadal Symptoms. J Urol. 2020;204(3):557–563.
➅ Matching Formulation To Patient Lifestyle And Adherence
Formulation matching should begin with the patient’s actual day-to-day life rather than with abstract preferences about route alone. Travel patterns, shift work, privacy, skin sensitivity, tolerance for injections, household transfer risk, cost, and ability to return for monitoring all shape whether a regimen is likely to succeed. Choosing the right formulation early reduces preventable instability and makes later interpretation more defensible because the clinical reasoning is clear from the beginning. [1-5]
A patient who travels frequently may struggle with storage requirements or predictable draw timing. A patient with an inconsistent daily routine may perform poorly on a therapy that requires precise daily execution. A patient who is highly sensitive to symptomatic peaks and troughs may need a delivery system that prioritizes steadier exposure over convenience alone. Matching formulation to lifestyle is therefore not a secondary comfort issue. It is a practical risk-reduction strategy that helps prevent avoidable instability later. [1-5]
➆ Monitoring, Side Effects, And Switching Strategies
Monitoring should reflect the formulation actually being used rather than follow a one-size-fits-all pattern. Injection regimens need a clearly defined point in the dosing interval for repeat labs. Transdermal regimens require consistent timing relative to application. Pellet regimens are interpreted over longer horizons, and oral regimens also require consistent timing relative to dosing routine. Without those rules, apparent treatment changes may reflect timing error rather than a real clinical shift. [1-5]
Side effects should be interpreted through pattern recognition whenever possible. Edema, irritability, insomnia, acne, and perceived wearing-off symptoms may each have kinetic fingerprints. When symptoms cluster after administration, the peak may need to be softened. When symptoms cluster late in the interval, adherence or interval length may be the main issue. When complaints do not track with dosing at all, clinicians should widen the lens to sleep, stress, stimulants, psychiatric factors, underground lab androgen use, and medical comorbidities before assuming testosterone is the primary cause. [1-5]
Switching is best handled in a staged way. Define the problem clearly, change one major variable at a time, reset the monitoring rules, and allow a stable observation window before judging the result. This approach reduces attribution confusion and preserves continuity when patients later move between clinicians or clinics. It also keeps the record far more useful than a sequence of rapid, overlapping changes. [1-5]
COURSE SUMMARY
Formulation choice plays a major role in testosterone therapy outcomes because it shapes pharmacokinetics, adherence, symptom stability, and the interpretability of follow-up. Injectable, transdermal, pellet, and oral therapies can all be effective, but each carries distinct strengths and limitations related to dosing interval, absorption, adjustability, and patient routine. Many apparent treatment failures are actually formulation mismatches, execution problems, or lab-timing problems rather than proof that total exposure is inadequate. Clinicians who understand peak-trough dynamics, steady-state timing, and adherence realities are better positioned to interpret symptoms and make rational adjustments. Matching the formulation to the patient’s life and monitoring it consistently produces safer and more stable testosterone care. [1-11]
Recommended Grand Rounds Case Reviews


Advanced Clinical Training Insights
Insightful articles that expand upon the Advanced Clinical Training Program, offering deeper exploration of testosterone, androgen, and hormone-related health topics to support disciplined clinical reasoning and real-world application.
New articles are published every week and will be incorporated on the individual training course pages to augment the learning.